Psychology Chapter 4 Important Question Psychological Disorders Term 2 2022
Class 12 Psychology Chapter 4 Important Question Psychological Disorders Term 2 2022, (Psychology) exams are Students are taught thru NCERT books in some of the state board and CBSE Schools. As the chapter involves an end, there is an exercise provided to assist students to prepare for evaluation. Students need to clear up those exercises very well because the questions inside the very last asked from those.
Sometimes, students get stuck inside the exercises and are not able to clear up all of the questions. To assist students, solve all of the questions, and maintain their studies without a doubt, we have provided a step-by-step NCERT Important Questions for the students for all classes. These answers will similarly help students in scoring better marks with the assist of properly illustrated Notes as a way to similarly assist the students and answer the questions right.
Class 12 Psychology Chapter 4 Important Question Psychological Disorders Term 2 2022
(A) Objective Questions (1 Marks Each)
Stand Alone MCQs
Q. 1. The other name for Multiple Personality Disorder
(A) Split Personality
(B) Dissociative Fugue
(C) Depersonalisation
(D) Dissociative Identity Disorder
Ans. Option (D) is correct.
Explanation: Dissociative Identity Disorder, often referred to as Multiple Personality, is the most dramatic of the dissociative disorders. It is often associated with traumatic experiences in childhood. In this disorder, the person assumes alternate personalities that may or may not be aware of each other.
Q. 2. Rhea always complains of snakes crawling inside her body. What is she suffering from?
(A) Somatic Hallucination
(B) Tactile Hallucination
(C) Delusion of Reference
(D) Delusion of control
Ans. Option (A) is correct.
Explanation: When a person has somatic hallucination, he/she experiences sensations within the body such as snake crawling inside one’s stomach.
Q.3. Aarav believes that he is being spied on, he feels threatened and victimised. He is suffering from
(A) Delusion of Control
(B) Delusion of Persecution
(C) Delusion of Grandeur
(D) Delusion of Reference
Ans. Option (B) is correct.
Explanation: Delusion of Persecution is the most common symptom of schizophrenia. People with this delusion believe that they are being plotted against, spied on slandered.
Q. 4. Inventing new words or phrases is called
(A) Neologism (B) Mutism
(C) Alogia (D) Perseveration.
Ans. Option (A) is correct.
Q. 5. The word diathesis refers to.
(A) Maintaining factor (B) Predisposition
(C) Genetic Factor (D) Environment
Ans. Option (B) is correct.
Explanation: The diathesis-stress model. This model states that psychological disorders develop when a diathesis (biological predisposition to the disorder) is set off by a stressful situation.
Q. 6. Alogia refers to.
(A) Loosening of association
(B) No emotion
(C) Poverty of speech
(D) Speed reduction
Ans. Option (C) is correct.
Explanation: Poverty of Speech Refers to reduction in speech and speech content.
Q. 7. Bullying is a type of ______ aggression.
(A) Physical (B) Verbal
(C) Proactive (D) Hostile
Explanation: Children show many different types of aggressive behaviour, example proactive aggression (i.e., dominating and bullying others without provocation).
Q. 8. _____ is vague, unpleasant feeling of apprehension.
(A) Panic (B) Anxiety
(C) Depression (D) Sadness
Ans. Option (B) is correct.
Explanation: Anxiety is usually defined as a diffuse, vague, very unpleasant feeling of fear and apprehension. The anxious individual also shows combination of the following symptoms: rapid heart rate, shortness of breath, diarrhoea, loss of appetite, fainting, dizziness, sweating, sleeplessness, frequent urination and tremors.
Q. 9. Excess activity of Dopamine causes.
(A) Depression (B) Anxiety
(C) OCD (D) Schizophrenia
Ans. Option (D) is correct.
Explanation: Excess of Dopamine is related to the schizophrenic disorder.
Q. 10. Match the following:
|
a. Tactile hallucination |
1. Food or drink taste strange. |
|
b. Auditory hallucination |
2. Smell of smoke. |
|
c. Visual hallucination |
3. Vague perception of colour/object. |
|
d. Gustatory hallucination |
4. Hears voices. |
|
e. Olfactory hallucination |
5. Forms of tingling and burning. |
(A) 1-e, 2-c, 3-b, 4-d, 5-a
(B) 1-b, 2-d3-c, 4-a, 5-e
(C) 1-e, 2-d, 3-c, 4-b, 5-a
(D) 1-d, 2-e, 3-c, 4-b, 5-a
Ans. Option (D) is correct.
Q. 11. A patient in the ward is maintaining an upright posture for hours and refuses to respond. Identify the kind of symptom.
(A) Catatonia Rigidity (B) Catatonia Stupor
(C) Catatonia Posturing (D) None of the above
Ans. Option (A) is correct.
Explanation: People with schizophrenia also show psychomotor symptoms. Some show catatonic rigidity, i.e., maintaining a rigid, upright posture for hours.
Q. 12 ______ is removing the evil that resides in the individual through counter magic and prayer.
(A) Decorcism (B) Reportism
(C) Exorcism (D) None of these
Ans. Option (C) is correct.
Explanation: Exorcism, i.e., removing the evil that resides in the individual through counter magic and prayer, is still commonly used. In many societies, the shaman, or medicine man (ojha) is a person who is believed to have contact with supernatural forces and is the medium through which spirits communicate with human beings.
Q. 13. Inability to stop thinking about a particular idea or topic is known as___________ behaviour.
(A) Obsessive (B) Repulsive
(C) Compulsory (D) Biological
Ans. Option (A) is correct.
Explanation: Obsessive behaviour is the inability to stop thinking about a particular idea or topic. The person involved, often finds these thoughts to be unpleasant and shameful.
Q. 14. When the person has to use more and more of a substance to get the same effect, is called________ .
(A) Substance dependence
(B) Substance abuse
(C) Tolerance
(D) Withdrawal
Ans. Option (C) is correct.
Explanation: When the person has to use more and more of a substance to get the same effect, it is called tolerance.
Q. 15. Myra keeps organising her cupboard the whole day. Even the thought of somebody messing it, keeps her distracted in class and makes her anxious. Such symptoms are typical of which disorder?
(A) Anxiety Disorder
(B) Depression
(C) Obsessive Compulsive Disorder
(D) Bipolar Disorder
Ans. Option (C) is correct.
Explanation: Myra has both obsession and compulsion of cleanliness. The thought of messy surroundings makes her anxious which shows her obsession/preoccupation with those thoughts. She also cleans her cupboard whole day which shows compulsive behaviour.
Q. 16. When a person’s overall behaviour patterns are inflexible and maladaptive and cause distress, the person may be diagnosed with:
(A) Schizophrenia
(B) Dissociative Identity Disorder
(C) A Personality Disorder
(D) Fugues
Ans. Option (C) is correct.
Assertion and Reason Based MCQs
Directions: In the following questions, a statement of Assertion (A) is followed by a statement of Reason (R). Mark the correct choice as:
(A) Both (A) and (R) are true, and (R) is the correct explanation of (A).
(B) Both (A) and (R) are true, but (R) is not the correct explanation of (A).
(C) (A) is true, but (R) is false.
(D) (A) is false, but (R) is true.
Q. 1. Assertion (A): Many psychologists believe that the best criterion for determining the normality of behaviour is not whether society accepts it, but whether it fosters the well-being of the individual and eventually of the group to which he/she belongs.
Reason (R): Health is not simply maintenance and survival, but also includes growth and fulfilment.
Ans. Option (C) is correct.
Explanation: Maintenance and survival with growth and development is called well-being and not health.
Q. 2. Assertion (A): The stigma attached to mental illness means that people are open to consult a doctor or psychologist.
Reason (R): It is commonly believed that psychological disorder is something to be ashamed of.
Ans. Option (D) is correct.
Explanation: The humiliation or stigma attached to mental illness means that people are hesitant or ashamed to consult a doctor or a psychologist.
Q. 3. Assertion (A): A classification of disorders consists of a list of categories of specific psychological disorders grouped into various classes on the basis of some shared characteristics.
Reason (R) : Classifications are useful because they enable users like psychologists, psychiatrists and social workers to communicate with each other about the disorder and help in understanding the causes of psychological disorders and the processes involved in their development and maintenance.
Ans. Option (B) is correct.
Explanation: Both the statements are true, but there is no cause and effect relationship between the two.
Q. 4. Assertion (A): The diathesis-stress model states that psychological disorders develop when a diathesis (biological predisposition to the disorder) is set off by a faulty gene.
Reason (R): The diathesis or the presence of some biological aberration which may be inherited.
Ans. Option (D) is correct.
Explanation: The psychological disorder develops not only because of faulty gene, but also by stressful situation. The diathesis-stress model states that psychological disorders develop when a diathesis (biological predisposition to the disorder) is set off by the stressful situation.
Q. 5. Assertion (A): Suicidal behaviour indicates difficulties in problem-solving, stress management and emotional expression. Suicidal thoughts lead to suicidal action only when acting on these thoughts seems to be the only way out of a person’s difficulties.
Reason (R): The stigma surrounding suicide continues despite recent advances in research in this field. Due to this, many people who are contemplating or even attempting suicide do not seek help thus, preventing timely help from reaching them.
Ans. Option (A) is correct.
Explanation: Often, suicidal behaviour indicates difficulties in problem-solving, stress management and emotional expression. Suicidal thoughts lead to suicidal action only when acting on these thoughts seems to be the only way out of a person’s difficulties. These thoughts are heightened under acute emotional and other distress. The ramifications of suicide on social circle and communities tend to be devastating and long-lasting.
Q. 6. Assertion (A): Genetic make-up or heredity is an important risk factor for major depression and other depressive disorders.
Reason (R): Depression is caused only by biological causes.
Ans. Option (C) is correct.
Explanation: Biological causes are not the only cause of depression. The psychological and social factors also contribute to depression.
Case-Based MCQs
I. Read the following text and answer the following questions on the basis of the same:
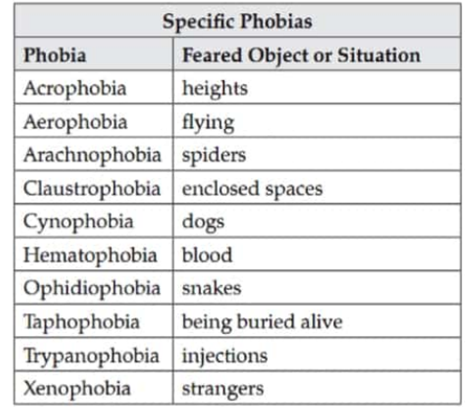
Phobia is a Greek word that means fear. A person diagnosed with a specific phobia (formerly known as simple phobia) experiences excessive, distressing and persistent fear or anxiety about a specific object or situation (such as animals, enclosed spaces, elevators or flying) (APA, 2013). Even though people realize their level of fear and anxiety in relation to the phobic stimulus is irrational, some people with a specific phobia may go to great lengths to avoid the phobic stimulus (the object or situation that triggers the fear arid anxiety). Typically, the fear and anxiety a phobic stimulus elicits is disruptive to the person’s life. For example, a man with a phobia of flying might refuse to accept a job that requires frequent air travel, thus negatively affecting his career. Clinicians who have worked with people who have specific phobias have encountered many kinds of phobias, some of which are shown in Table
Specific phobias are common; in the United States, around 12.5% of the population will meet the criteria for a specific phobia at some point in their lifetime (Kessler et al., 2005). One type of phobia, agoraphobia, is listed in the DSM-5 as a separate anxiety disorder. Agoraphobia, which literally means “fear of the marketplace,” is characterised by intense fear, anxiety and avoidance of situations in which it might be difficult to escape or receive help if one experiences symptoms of a panic attack (a state of extreme anxiety that we will discuss shortly). These situations include public transportation, open spaces (parking lots), enclosed spaces (stores), crowds or being outside the home alone (APA, 2013). About 1.4% of Americans experience agoraphobia during their lifetime (Kessler et al., 2005)
Q. 1. What is the Greek word for “Phobia”?
(A) Fear (B) Experience
(C) Body (D) None of these
Ans. Option (A) is correct.
Q. 2. The fear of strangers is called:
(A) Xenophobia (B) Taphephobia
(C) Cynophobia (D) Aerophobia
Ans. Option (A) is correct.
Q. 3. What is “Phobia”?
(A) An extreme or irrational fear of or aversion to something.
(B) An unpleasant emotion caused by the threat of danger, pain or harm.
(C) A feeling of worry, nervousness or unease about something with an uncertain outcome.
(D) None of these
Ans. Option (A) is correct.
II. Read the following text and answer the questions given below:
Anxiety Disorder: The term anxiety is defined as diffuse, vague and very unpleasant feeling of fear and apprehension. The anxious individual shows a combination of following symptoms: Rapid heart rate, shortness of breath, diarrhoea, loss of appetite, fainting, dizziness, sweating, sleeplessness, frequent urination and tremors.
Obsessive-Compulsive and Related Disorders: People with OCD are unable to control their preoccupations with specific ideas or are unable to prevent themselves from repeatedly carrying out a particular act, which affects their ability to carry out normal activities. Obsessive Behaviour- Inability to stop thinking about a particular idea or topic.
Compulsive Behaviour- It is the need to perform certain behaviours over and over again. For e.g., Counting, touching, checking, washing, etc. E.g., Hoarding Disorder, Trichotillomania (hair pulling disorder), Excoriation (skin picking).
Trauma and Stress-Related Disorder: People who are caught in natural disasters, bomb blasts or have been in serious accidents, or in a war situation, experience post-traumatic stress disorder (PTSD).
Symptoms- Recurrent dreams, flashbacks, impaired concentration & emotional numbing. Includes- Adjustment disorder and Acute Stress Disorder.
Somatic Symptom and Related Disorder- All conditions in which there are physical symptoms in the absence of a physical disease. The individual has psychological difficulties & complains of physical symptoms, for which there is no biological cause.
Q. 1. What is anxiety?
(A) It is defined as diffuse, vague and very unpleasant feeling of fear and apprehension.
(B) An extreme or irrational fear of or aversion to something.
(C) An unpleasant emotion caused by the threat of danger, pain or harm.
(D) None of these
Ans. Option (A) is correct.
Q. 2. What are the symptoms of anxious people?
(A) Loss of appetite (B) Fainting
(C) Dizziness (D) All of the above
Ans. Option (D) is correct.
Q. 3. Compulsive behaviour is doing things over and over again like:
(A) Counting (B) Touching
(C) Checking (D) All of the above
III. Read the following text and answer the questions given below:
Mr. Sen is a 67-year-old male who reports that his biggest problem is worrying. He worries all of the time and about “everything under the sun.” For example, he reports equal worry about his wife who is undergoing treatment for breast cancer and whether he returned his book to the library. He recognizes that his wife is more important than a book and is bothered that both cause him similar levels of worry. Mr. Sen is unable to control his worrying. Accompanying this, he experienced excessive and uncontrollable anxiety, had difficulty falling asleep, impatience with others, difficulty focusing at work, and significant back and muscle tension. Mr. Sen has had a lifelong problem with worry, recalling that his mother called him a “worry wart.” His worrying does wax and wane, and worsened when his wife was recently diagnosed with breast cancer.
Q. 1. Identify Mr. Sen’s disorder.
(A) Generalized Anxiety Disorder
(B) Major Depressive Disorders
(C) Obsessive- Compulsive Disorder
(D) Somatic Symptom Disorder
Ans. Option (A) is correct.
Explanation: Generalised Anxiety Disorder consists of prolonged, vague, unexplained and intense fears that are not attached to any particular object.
Q. 2. Identify the odd one out:
(A) Specific Phobias
(B) Social Anxiety Disorder
(C) Obsessive Compulsive Disorder
(D) Generalized Anxiety Disorder
Ans. Option (C) is correct.
Explanation: Rest all are under Anxiety Disorder Spectrum.
Q. 3. What is the nature of fear experienced by a person suffering from generalised anxiety disorder?
(A) Irrational (B) Mild
(C) Unexplained terror (D) None of the above
Ans. Option (C) is correct.
Q. 4. According to Behavioural model, Mr. Sen’s symptoms are due to:
(A) Irrational assumptions
(B) Maternal deprivation
(C) Learned maladaptive ways of behaving
(D) Inability to find meaning in life
Ans. Option (C) is correct.
Explanation: As per Behavioural model both normal and abnormal behaviours are learned and psychological disorders. They are the result of learning maladaptive ways of behaving. The model concentrates on behaviours that are learned through conditioning and proposes that what has been learned can be unlearned.
(B) Subjective Questions
Very Short Answer Type Questions (2 Marks Each)
Q. 1. What is an interactional approach to psychological disorders ? [CBSE Delhi Set-4, 2018]
Ans. Interactional approach to psychological disorders:
(a) Bio-psycho – social approach
(b) All three factors i.e., biological, psychological and social, play important role in influencing the expression and outcome of psychological disorders.
Q. 2. Explain separation anxiety disorder (SAD). [CBSE Delhi Set-4, 2018]
Ans. Separation anxiety disorder – an internalising / behavioural disorder unique to children
OR
Symptoms prominent symptom is excessive anxiety/ panic experienced by children at being separated from their parents, difficulty being in a room by themselves, going to school alone, fearful of entering new situations and clings to and shadow their parents’ every move. To avoid separation, children with SAD may fuss, scream, throw severe tantrums or make suicidal gestures.
Q. 3. Explain binge eating. [CBSE OD Set-4, 2017]
Ans. In binge eating, there are frequent episodes of out of control eating.
Detailed Answer:
Binge Eating is also known as compulsive overeating or consuming abnormal amounts of food while feeling inability to stop and a loss of control. Binge eating generally occurs on an average a minimum of twice per week for a duration of six months. This phenomenon was first explained in 1959 by Albert Stunkard, a psychiatrist and researcher, as Night Eating Syndrome (NES). The term ‘Binge Eating’ was created to define similar eating behaviour irrespective of the nocturnal incidents.
Q. 4. What is bipolar mood disorder? [CBSE Delhi, 2016]
Ans. Bipolar Mood Disorder: hr this, both mania and depression are alternatively present and are interrupted by periods of normal mood.
Manic episodes rarely appear by themselves; they usually alternate with depression. Bipolar mood disorders were earlier referred to as manic- depressive disorders.
Q. 5. Fatima is experiencing generalised anxiety disorder. Enumerate any two causes with reference to diathesis stress model which may have led to the disorder. [CBSE SQP 2020-2021]
Ans. (i) Presence of biological aberration
(ii) Person may carry a vulnerability
(iii) Presence of pathogenic stressors
(Explain any two relating to the case provided)
Detailed Answer:
(i) The diathesis or the presence of some biological aberration which may be inherited.
(ii) The diathesis may carry a vulnerability to develop a psychological disorder. This means that the person is ‘at risk’ or ‘predisposed’ to develop the disorder.
(iii) The presence of pathogenic stressors, i.e. factors/ stressors that may lead to psychopathology.
Short Answer Type Questions-I (3 Marks Each)
Q. 1. Describe Dissociative Disorders.
Ans. Dissociation can be viewed as a severe connection between ideas and emotions.
Dissociation involves feelings of unreality, estrangement, depersonalisation and sometimes a loss or shift of identity.
Four conditions are included in this group:
(i) Dissociative amnesia: It is characterised by extensive but selective memory loss that has no known organic cause (e.g., head injury).
(ii) Dissociative fugue: It has, as its essential feature, an unexpected travel away from home and workplace, the assumption of a new identity, and the inability to recall the previous identity.
(iii) Dissociative identity disorder: It is often referred to as multiple personality, is the most dramatic of the dissociative disorders. It is often associated with traumatic experiences in childhood.
(iv) Depersonalisation: It involves a dreamlike state in which the person has a sense of being separated both from self and from reality.
Q. 2. How does diathesis stress model explain abnormal behaviour?
Ans. The three components of diathesis stress model are:
(i) Diathesis or the presence of some biological aberration which may be inherited.
(ii) The person may carry a vulnerability to develop a disorder. The person is ‘at risk’ or ‘predisposed’ to develop the disorder.
(iii) There is a presence of pathogenic stressors that may lead to psychopathology.
Q. 3. Explain the forms of eating disorders associated with distorted body image.
Ans. Children show eating disorders which are of the following three types:
(i) Anorexia Nervosa: In this, the individuals have a distorted body image that leads them to consider themselves as overweight. They refuse to eat especially, in front of others, exercise compulsively and lose large amounts of weight and even starve themselves to death.
(ii) Bulimia Nervosa: In this, the individual may eat excessive amounts of food, then purge his/her body of food by using medicines or by vomiting. The person feels disgusted and ashamed when he or she binges and is relieved of tension and negative emotions after purging.
(iii) Binge Eating: In this, there are frequent episodes of out-of-control eating. Large amount of food is eaten even when the individual is not feeling hungry.
Short Answer Type Questions-ll (4 Marks Each)
Q. 1. Aman is an eight year old who has profound difficulty in relating to other people. Often, he is found to be unresponsive to other people’s feelings and exhibits stereotypical patterns of behaviour. Identify this disorder and describe its features. [CBSE Delhi Set-4, 2019]
Ans. Autism Spectrum Disorder under the category of Neuro developmental disorders
Children with autism spectrum disorder have marked difficulties in social interaction and communication.
• They have a restricted range of interests.
• They have a strong desire for routine.
• They are unable to share experiences and emotions.
• They show serious abnormalities in communication and language that persist over time.
• Many never develop speech, those who do have repetitive deviant patterns.
• They show narrow patterns of interests and repetitive behaviours such as lining up objects or stereotyped body movements.
(Any 3 points from above other than the ones mentioned in the question)
Q. 2. Explain mental disorders from a socio-cultural perspective. [CBSE OD Set-4, 2017]
Ans. According to the Sociocultural model, abnormal behaviour is best understood in light of the social and cultural forces that influence an individual.
(i) Socio-cultural factors such as war and violence, group prejudice and discrimination, economic and employment problems, etc. and rapid social change, put stress on most of us and can lead to psychological problems in some individuals.
(ii) Certain family structures are likely to produce abnormal functioning in members. E.g., families which are over involved with each other have difficulty in becoming independent in life. Social and professional relationships also play an important role.
(iii) People who are isolated and lack societal support are likely to become more depressed and remain depressed longer than those who have good friendship.
(iv) Societal labels and roles assigned to troubled people also cause abnormal functioning.
OR
When people break the norms of their society, they are called deviant and ‘mentally ill’ and people may start behaving and living up to these labels.
Q. 3. Explain somatoform disorders. [CBSE Delhi, 2015]
Ans. Somatoform Disorders: Physical symptoms in the absence of a physical disease. Individuals have psychological difficulties and complains of physical symptoms for which no biological cause exists. E.g., fatigue, headache, vague body pains.
Types:
(a) Pain disorders
(b) Somatisation
(c) Conversion
(d) Hypochondriasis
Brief explanation with symptoms of each disorder.
Detailed Answer:
In somatoform disorders, the individual has psychological difficulties and complains of physical symptoms, for which there is no biological cause, i.e., absence of a physical disease.
Somatoform disorders include:
(a) Pain disorder: It involves reports of extreme and incapacitating pain, that is without any identifiable biological symptoms or greatly in excess of what might be expected to accompany biological symptoms. Some people handle pain by remaining active and ignoring the pain. Others engage in passive coping, which leads to reduced activity and social withdrawal.
(b) Somatisation disorder: Patients with somatisation have multiple recurrent chronic bodily complaints. These complaints are likely to be presented in a dramatic and exaggerated way. Common complaints are headache, fatigue, heart palpitations, fainting spells, vomiting and allergies. Patients with this disorder believe that they are sick, provide long and detailed histories of their illness, and take large quantities of medicine.
(c) Conversion disorder: Patients with conversion disorder mainly report loss of part or all of some basic body functions. Paralysis, blindness, deafness and difficulty in walking are generally among the symptoms reported.
(d) Hypochondriasis: Patient with hypochondriasis disorder has a persistent belief that she/he has a serious illness, despite medical reassurance, lack of physical findings and failure to develop the disease. Hypochondriacs have an obsessive preoccupation and concern with the condition of their bodily organs and they continually worry about their health.
Q. 4. Raj can often be seen talking to himself. On questioning, he would state that there were people around him whom he could see and hear when there was no one else around. Identify and describe this symptom of schizophrenia. [CBSE SQP 2020-2021]
Ans. Positive symptom Hallucinations are perceptions that occur in the absence of external stimuli, positive symptoms of schizophrenia.
Auditory and visual hallucination
Listing and description of other types of hallucinations.
Detailed Answer:
(i) People with schizophrenia may have hallucinations, i.e. perceptions that occur in the absence of external stimuli. Auditory hallucinations are most common in schizophrenia. Patients hear sounds or voices that speak words, phrases and sentences directly to the patient (second person hallucination) or talk to one another referring to the patient as she/he (third person hallucination).
(ii) Hallucinations can also involve the other senses. These include tactile hallucinations (i.e. forms of tingling, burning), somatic hallucinations (i.e. something happening inside the body such as a snake crawling inside one’s stomach), visual hallucinations (i.e. vague perceptions of colour or distinct visions of people or objects), gustatory hallucinations (i.e. food or drink taste strange), and olfactory hallucinations (i.e. smell of poison or smoke).
(iii) People with schizophrenia also show inappropriate affect, i.e. emotions that are unsuited to the situation.
Q. 5. What are dissociative disorders? Explain their various types.
OR
Explain disruptive, impulse-control and conduct disorders.
Ans. Sudden temporary alterations of consciousness that block out painful experiences. Severance of connection between ideas and emotions, feelings of unreality, loss or shift of identity.
(i) Dissociative Amnesia
(ii) Dissociative identity disorder
(iii) Depersonalization/ Derealisation
(Explanation of the above. In case only the names of disorders are written without explaining, marks to be given).
OR
Oppositional Defiant Disorder displays age – inappropriate amounts of stubbornness, are irritable, defiant disobedient and behave in a hostile manner. Individuals with ODD do not see themselves as angry, oppositional or defiant and often justify their behaviour as reaction to circumstances/ demand, problematic interactions with others. (Any four points to be written)
Conduct Disorder and antisocial behaviour refer to age – inappropriate actions, and attitude that violate family expectations, societal norm and the personal or property rights of others. Include aggressive actions that cause or threaten harm to people or animals, non- aggressive conduct that causes property damage, major deceitfulness or theft and serious role violations. Children show many different types of aggressive behaviour Such as verbal aggression, physical aggression, hostile aggression and proactive aggression. (Any four points to be written)
Long Answer Type Questions (6 Marks Each)
Q. 1. Explain abnormality. Trace a brief history of how our understanding of psychological disorders has evolved to its current status.
OR
Explain the different psychological models used to explain abnormal behaviour. [CBSE Delhi Set-4, 2019]
Ans. (i) Deviance Two approaches
(ii) Distress OR Deviation from social norms.
(iii) Dysfunction maladaptive behaviour
(iv) Danger
(Explanation of the above)
(Second part, ‘historical background’, not in curriculum 2018-19, therefore, everyone would get marks).
OR
Psychological models-These factors include maternal deprivation, faulty parent child relationships, maladaptive family structures and severe stress.
Model
(i) Psychodynamic
(ii) Behavioural model
(iii) Cognitive model
(iv) Humanistic model
(Explanation of all 4 models / 7/2 for each model)
Detailed Answer:
Psychological models maintain that psychological and interpersonal factors have a significant role to play in abnormal behaviour. These factors include:
(i) Maternal deprivation (separation from the mother, or lack of warmth and stimulation during early years of life).
(ii) Faulty parent-child relationships (rejection, over protection, over-permissiveness, faulty discipline, etc.)
(iii) Maladaptive family structures (inadequate or disturbed family) and severe stress. The psychological models include the psychodynamic, behavioural, cognitive and humanistic-existential models.
(a) The Psychodynamic Model: This model is the oldest and most famous of the modern psychological-models. Abnormal behaviour is viewed as the result of intrapsychic conflicts.
1. This model was first formulated by Freud.
2. Abnormal behaviour is a symbolic expression of unconscious mental conflicts that can be generally traced to early childhood or infancy.
(b) The Behavioural Model: This model states that both normal and abnormal behaviours are learned and psychological disorders are the result of learning maladaptive ways of be having. The model concentrates on behaviours that are learned through conditioning and proposes that what has been learned can be unlearned. Learning can take place by classical conditioning (temporal association in which two events repeatedly occur close together in time), operant conditioning (behaviour is followed by a reward) and social learning (learning by imitating others’ behaviour). These three types of conditioning account for behaviour, whether adaptive or maladaptive.
(c) The Cognitive Model: This model states that abnormal functioning can result from cognitive problems like negative thinking and irrational believes. People may hold assumptions and attitudes about themselves that are irrational and inaccurate. People may also repeatedly think illogical ways and make over generalizations. They may draw broad, negative conclusions on the basis of a single insignificant event.
(d) The Humanistic-Existential Model: Humanists believe that human beings are born with a natural tendency to be friendly, co-operative and constructive, and are driven to self actualize, i.e., to fulfil this potential for goodness and growth. Existentialists believe that from birth we have total freedom to give meaning to our existence or to avoid that responsibility. Those who shirk from this responsibility would live empty, inauthentic and dysfunctional lives. According to humanists, obstacles in self actualization cause mental disorder.
Q. 2. Explain the term dissociation. Discuss its various forms. [CBSE OD Set-4,2016]
Ans. Dissociation: Severance of the connection between ideas and emotions. Involves feelings of unreality, estrangement, depersonalisation and sometimes a loss or shift of identity.
Forms of dissociative disorders are:
(i) Dissociative amnesia
(ii) Dissociative fugue
(iii) Dissociative identity disorder
(iv) Depersonalisation
(Explanation of each)
Detailed Answer:
(i) Dissociative amnesia is characterised by extensive but selective memory loss that has no known organic cause (e.g., head injury). Some people cannot remember anything about their past. Others can no longer recall specific events, people, places, or objects, while their memory for other events remains intact.
(ii) A part of dissociative amnesia is dissociative fugue. Essential feature of this could be an unexpected travel away from home and workplace, the assumption of a new identity, and the inability to recall the previous identity. The fugue usually ends when the person suddenly ‘wakes up’ with no memory of the events that occurred during the fugue. This disorder is often associated with an overwhelming stress.
(iii) Dissociative identity disorder, often referred to as multiple personality, is the most dramatic of the dissociative disorders. It is often associated with traumatic experiences in childhood. In this disorder, the person assumes alternate personalities that may or may not be aware of each other.
(iv) Depersonalisation/Derealisation disorder involves a dreamlike state in which the person has a sense of being separated both from self and from reality. In depersonalisation, there is a change of self-perception, and the person’s sense of reality is temporarily lost or changed.
Q. 3. Explain the diathesis-stress model of abnormal behaviour giving examples from daily life. [CBSE OD Set-4, 2016]
Ans. Diathesis Stress Model: This model states that psychological disorders develop when a diathesis (biological aberration to the disorder) is set off by a stressful situation.
This model has three components:
(i) Presence of some biological aberration which may be inherited.
(ii) Diathesis may carry predisposition or vulnerability to develop a psychological disorder.
(iii) Presence of pathogenic stressors i.e., factors that may lead to psychopathology.
(Any suitable example from daily life)
Detailed Answer:
Diathesis-stress model: This model states that psychological disorders develop when a diathesis (biological predisposition to the disorder) is set off by a stressful situation. This model has three components. The first is the diathesis or the presence of some biological aberration which maybe inherited. The second component is that the diathesis may carry a vulnerability to develop a psychological disorder. This means that the person is ‘at risk’ or ‘predisposed’ to develop the disorder. The third component is the presence of pathogenic stressors, i.e. factors/ stressors that may lead to psychopathology. If such “at risk” persons are exposed to these stressors, their predisposition may actually evolve into a disorder. This model has been applied to several disorders including anxiety, depression, and schizophrenia.
Q. 4. Describe any three behavioural disorders prevalent among children.
Ans. The most important three behavioural disorders among children are Attention-Deficit Hyperactivity Disorder, Oppositional Defiant Disorder and Conduct Disorder.
Attention Deficit Hyperactivity Disorder: The two main features of ADHD are Inattention and Hyperactivity.
Inattention: Children who are inattentive find it difficult to sustain mental effort during work or play.
They have a hard time keeping their minds on any one thing or in following instructions.
Common complaints are that the child does not listen, cannot concentrate, does not follow instructions, is disorganised, easily distracted, forgetful, does not finish assignments, and is quick to lose interest in what he and she feels to be boring activities.
Hyperactivity: Children showing hyperactivity are unable to control their reactions or think before they act. They are impulsive and find it impossible to sit still through a class. Minor mishaps like knocking things over or major mishaps like serious injury due to accident may occur.
They may fidget, squirm, climb, or run around aimlessly and talk incessantly.
They are described as “driven by motor” and “always on the go” by their parents and teachers.
Boys are four times more likely to be given this diagnosis than girls.
Oppositional Defiant Disorder: With Oppositional Defiant Disorder, they show age-inappropriate amount of stubbornness. They are irritable, defiant, disobedient and behave in a hostile manner.
Conduct Disorder: It refers to age inappropriate actions and attitudes that violate family expectations, societal norms and the personal or property rights of others. The behaviours typical of conduct disorder include aggressive actions that cause or threaten harm to people or animals, non-aggressive conduct that causes property damage, major deceitfulness or theft and serious rule violations.